
Estimated read time: 11-12 minutes
This archived news story is available only for your personal, non-commercial use. Information in the story may be outdated or superseded by additional information. Reading or replaying the story in its archived form does not constitute a republication of the story.
Editor’s note: These answers are based on interviews and information current as of the time of publication. Please be aware that new information may be discovered by health experts after publication. We’re working to keep this information as up-to-date as possible.
SALT LAKE CITY — Utah crossed the 30,000-case plateau this week as its number of COVID-19 cases remains at the highest rates since the pandemic began.
From its beginning, we’ve asked you, our readers, to submit questions about the coronavirus pandemic to us so we can dig up the answers for you. Here's a look into some statistics, where the spread is happening and answers to other questions you've sent us about the coronavirus.
What are the statistics we should be looking at?
First off, it should be noted that this is an amalgamation of about a half-dozen questions you’ve asked us about various statistics. We combined it into this question.
At the beginning of the pandemic, case counts were an important statistic. But since more than half of Utah’s over 30,000 cases are now considered recovered, that’s not as telling to the current situation as it once was. Instead, Dr. Angela Dunn, the state’s epidemiologist, said it’s important to look at the state’s seven-day rolling average case count.
“We’re now at a point, with this outbreak, where it’s more meaningful to look at the seven-day trends and percent positives of all of our tests,” she explained, during a press briefing last week. “This allows us to really identify meaningful trends in our data, and it decreases the noise from the day-to-day fluctuations we’re seeing.”
As of Tuesday, Utah had a seven-day rolling average of 635.7 cases with a 10.21% positive rate. Those were the average number of new cases and the percentage of positives per test daily in the past week. When placed on a graph, it shows on a better scale if new cases or positive rates of tests are increasing or decreasing.
The data shows exactly how Utah went from a seven-day average of 157 cases on Memorial Day and steadily rose to today's average, which is four times higher. It also shows how the average jumped from 4.9% to 10.2% through the same steady rise.
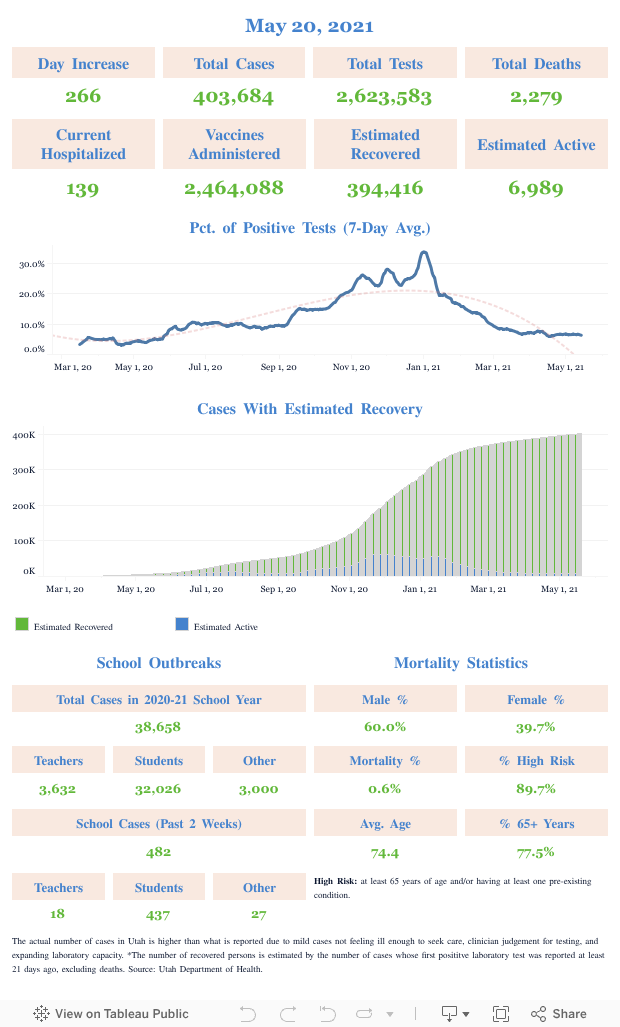
This, in turn, shows just how active the COVID-19 spread is in Utah now in comparison to what it was on Memorial Day. But it also shows the nuances within the rise that officials can go back and look to see what may have caused a spike or a dip in new cases or positive percentage during a specific time in the pandemic.
We reached out to the Utah Department of Health to see what other stats are important to know. Charla Haley, a spokesperson for the department, said officials are also looking closely at the number of deaths, hospitalizations and demographics of the people getting sick.
“The Utah Department of Health weighs many issues when making recommendations for mitigation efforts,” she said, in an email to KSL.com.
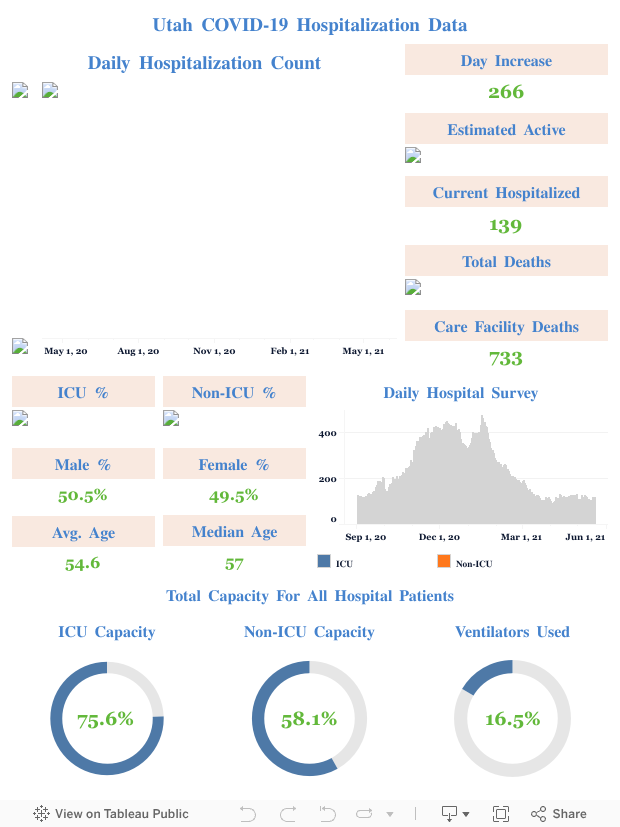
Last week, experts at hospitals explained the current situation at Utah hospitals and what the growing data means for hospitals if it continues. As of Tuesday, the state health department reported 45% capacity for all hospital beds and 65% capacity of intensive care units. That said, experts pointed out that if new cases continue to rise, hospitalizations may soon hit a critical point.
"We’re not making the headway we need to make with the plea to the public to be socially responsible, and it feels as (if) we’re headed for a disaster," Dr. Arlen Jarrett, chief medical officer with Steward Healthcare, said Friday. "It’s very clear that if we stay on this same path, we are going to maximize our hospital capacities very soon."
The state provides details about demographics on the state health department's website; however, it shows 39% of all cases in Utah involve people aged 25-44, which marks the largest age group for cases. But people aged 45-64 had the highest number of hospitalizations. It also shows an ongoing discrepancy within minority communities, which has been the case for months.
Where is this primarily being spread and contracted?
The state department’s latest map of COVID-19 spread over a 14-day period shows it’s spreading about everywhere in Utah and at high per capita rates — aside from Emery and Carbon counties, which 1 to 5 cases per 100,000 people in those areas combined. Hyrum was also listed in that category by health officials.
The department listed Duchesne County and Daggett and Uintah counties as being “moderate” rate areas over the past two weeks. That’s defined as over 10 to 50 cases per 100,000 people. Parts of central Utah — like Richfield, Monroe and Salina — had “moderately high” rates, which means over 50 to 100 cases per 100,000 people. Morgan County was also listed in that moderately high range.
The rest of the state was considered “high rate” over the past two weeks, which means more than 100 cases per 100,000 residents over that span.
The disease is still predominantly spread through known contacts in household settings. As of Tuesday, known contact with someone with COVID-19 accounts for nearly two-thirds of all Utah cases. And within those cases, contact within the household remains 61% of the causes. Only 13% of cases are attributed to community spread, which has remained constant through the uptick.
You can find recommendations on how to quarantine at home with housemates who are sick here.
Can you tell us city by city, within Salt Lake, what the numbers are?
State health department data does indeed have a breakdown in Salt Lake County. According to Johns Hopkins University data, Salt Lake County entered Tuesday with 40th-most cases of any county in the U.S. As of Tuesday, it has 15,083 cases.
It’s also been well documented already that West Valley City and the western part of Salt Lake City have been hit hard, which has led to measures by state officials to improve communication with individuals in the Latino-Hispanic and Pacific Islander communities.
So what’s the breakdown of all cases in the county through the state health department’s data Tuesday?
- West Valley City: 3,362
- Salt Lake City (all neighborhoods included): 2,946
- West Jordan/Copperton: 1,482
- Sandy: 838
- Taylorsville: 565
- Magna: 548
- Midvale: 515
- South Salt Lake: 512
- Herriman: 510
- Taylorsville/Murray (blended section): 496
- Murray: 494
- South Jordan (including Daybreak): 486
- Millcreek: 370
- Draper: 322
- Riverton/Bluffdale: 300
- Holladay: 236
- Cottonwood Heights: 221
- Other/not listed: 880
This data includes all cases since testing and counting began in March, but all locations in the county were listed as having high COVID-19 case rates over the past two weeks.
Which counties in Utah have had the most deaths?
It’s not surprising that areas with the most cases have the most deaths. For example, Salt Lake County has 49.5% of all cases and 57.5% of all Utah COVID-19 deaths, as of Tuesday. In all, Salt Lake County has reported 130 deaths, followed by Utah County with 29.
Centers for Disease Control and Prevention county data lists Box Elder, Cache, Davis, Garfield, Iron, San Juan, Summit, Wasatch, Washington and Weber counties as having fewer than 20 COVID-19 deaths; no deaths have been reported from Utah’s remaining 17 counties, according to CDC data.
Where does the research stand on getting COVID-19 a second time?
This has been addressed in a previous mailbag, but it remains among the top questions we continue to receive. Luckily, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, provided an update on this topic during a conversation with Dr. Francis Collins, the director of the National Institutes of Health, for TIME last week.
The answer remains the same: It’s unknown but unlikely. Fauci said there is no documented scientific case of someone contracting COVID-19, recovering, and then getting it again. He also said it’s not known if a future vaccine will offer long-term protection, or if it will have to be administered yearly like the flu vaccine.
“The idea of relapses — I wouldn’t be surprised if there’s a rare case of an individual who went into remission and relapsed. We saw that in ebola,” Fauci said, referring to the story of Pauline Cafferkey.
“I can say with confidence, that it’s very unlikely that it’s a common phenomenon that people recover (and get sick again),” he continued.
What is a "known contact"?
We reached out to the state health department for this question as they are the ones providing the statistics.
“Known contact means you are in close contact often with someone who has been diagnosed with COVID-19. And, in most cases, it means you ‘know’ where you were likely exposed,” Haley said.
What is an effective way to kill the coronavirus?
Assuming this is about cleaning, the Environmental Protection Agency has a guide of 432 cleaning products believed to be strong enough to kill viruses like the virus that causes COVID-19. The list made news last week when two Lysol products were confirmed to have killed the SARS-CoV-2 virus, which causes COVID-19.
Those were Lysol Disinfectant Max Cover Mist and Lysol Disinfectant Spray. According to the EPA, both products were able to kill the virus in 2 minutes.
Can I volunteer to help with contact tracing? Can I do it from home?
Haley said the state health department is not currently accepting volunteers for contact tracing. The department is, however, looking to hire Spanish-speaking contact tracers; anyone seeking to apply is encouraged to apply by sending their resume to Janae Duncan at the state health department. Contact tracers do work remotely, according to Haley.
How does a false negative happen, and can a person have COVID-19 in their body but test negative because the concentration of COVID-19 is not very high?
Haley explained that a negative test result means that SARS-CoV-2 was not found in the sample.
“For COVID-19, a negative test result for a sample collected while a person has symptoms usually means that COVID-19 did not cause your recent illness,” she said, adding that it is possible for an incorrect negative result to happen.
“This means that you might still have COVID-19 even though the test result is negative,” she said. “This can sometimes happen when someone has been exposed but didn't wait at least 7 days after that exposure to get tested.”
When will it be over?
This is likely a question we’ve all thought at least once over the past few months. While the recent surge in Utah and many other states are discouraging, there are signs of hope in the U.S. and elsewhere in the world.
For example, New York City officials on Monday celebrated its first 24-hour period without a death reported in months. That’s not to say COVID-19 is over in New York, but it’s a major moment for an area that was hit hardest when the COVID-19 pandemic first reached the U.S. Several European countries have reported slowdowns in cases as well.
By now, we’re all well aware that a vaccine is one of the more important factors to moving past COVID-19. During Fauci’s TIME interview last week, he pointed out that there were still “multiple candidates” in the vaccine race, and it’s possible that one of the candidates could reach Phase III, or the efficacy phase, by the end of this month. The Associated Press reported Tuesday that a vaccine developed by the National Institutes of Health and Moderna Inc. is slated to begin this phase on July 27.
It’s expected that at least three other candidates will reach that period by the end of October. In all, some 30,000 people are to participate in trials, according to Fauci.
“We hope by the end of this year or by the beginning of 2021, we will at least have an answer whether the vaccine or vaccines, plural, are safe and effective,” he said last week.
While it may take a few more months to have a viable vaccine, Fauci said that the medical field is working with manufacturers to make more doses now even though it’s unclear whether the vaccine works. This aspect is a bit of a gamble. If it’s determined that the vaccine isn’t safe or effective, those doses will have to be destroyed; but it also means if a vaccine is approved, there will be a larger supply of that vaccine to be distributed at that time.
“When we get to the winter and the early part of 2021, we will start to have a large number of doses that people will be able to use if it turns out to be safe and effective,” Fauci said.
That gamble, he added, is a financial risk but not a risk for safety or scientific integrity.
_If you have questions about the coronavirus, please submit them to the KSL.com Google response form below for future installments._
Submit Your Questions:







