Estimated read time: 3-4 minutes
This archived news story is available only for your personal, non-commercial use. Information in the story may be outdated or superseded by additional information. Reading or replaying the story in its archived form does not constitute a republication of the story.
SALT LAKE CITY — A standard reference tool used by the medical profession is so inaccurate that doctors across the country are accidentally killing patients by the thousands each year, according to an expert in Utah who co-authored a disturbing new study.
The study found that the faulty reference tool is responsible for a significant portion of the growing death toll from prescription painkillers.
"I think it could be thousands, nationally, for sure," said Dr. Lynn Webster of Lifetree Clinical Research in Salt Lake City. He believes dozens of Utahns die each year for the same reason.
They're notoriously inaccurate. In fact, I call them 'the death table.'
–- Dr. Lynn Webster
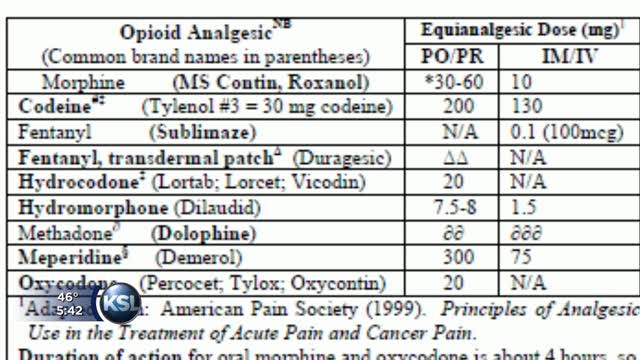
At issue are so-called "equianalgesic conversion tables." Physicians use the tables to calculate the proper dose when a patient is switching from one "opioid" painkiller to another. The tables display equivalent doses of various drugs.
"They're notoriously inaccurate," Webster said. "In fact, I call them 'the death table.'"
Webster and Dr. Perry G. Fine of the University of Utah co-authored the new study, which is a review of medical literature and forensic reports from around the country. It's published in the April edition of Pain Medicine, the official journal of the American Academy of Pain Medicine.
- 10 to 30% reduction of the original dose while the new drug is used at the lowest available dose.
- 10 to 25% reduction of the original drug each week while the new drug dosage is gradually increased
The study may cause a stir because of the prominence of the two researchers. Fine is immediate past-president of AAPM and Webster is the organization's president-elect.
"We've been taught that these equal analgesic tables are reasonably safe, as a guide," Webster said. "And they're not."
Patients who need pain medication frequently switch from one drug to another. Doctors often prescribe a change because of side- effects such as nausea. Patients also switch drugs because they develop a tolerance for a given painkiller or because insurance companies won't continue covering an expensive drug.
The prescribing physician typically figures out the proper equivalent dose by consulting the published conversion tables.
They're often flat wrong, according to Webster.
"And that's why we're basically on a campaign nationally to make sure that every physician who prescribes an opioid understands they can't use these conversion tables," he said.
We're basically on a campaign nationally to make sure that every physician who prescribes an opioid understands they can't use these conversion tables.
–- Dr. Lynn Webster
Nationally, an estimated 15,000 people die each year from overdoses of opioid pain medicine. That includes such familiar painkillers as Oxycontin, oxycodone, Percocet, morphine, and methadone.
"A lot of the deaths have been attributed to using these conversion tables and starting patients on too high of a dose," Webster said.
"Methadone is the riskiest," he said, but all the opioids can be deadly if the prescribing physician gets the dosage wrong.
He emphasizes that it's not just drug addicts and long- term patients who are at risk.
"It could be somebody who's been on pain medication after a hip operation or a knee operation for several weeks and it's not working any more," Webster said. When a physician uses the conversion tables to estimate the proper dose, "It could be very far off from what's safe."
As a solution to the problem, Webster recommends that a prescribing physician gradually phase in the new drug instead of abruptly switching from one to the other. He said the original dose should be reduced by 10 to 30 percent while the new drug is used at the lowest available dose. Then the original drug should be reduced by 10 to 25 percent each week while the new drug dosage is gradually increased.
Webster says physicians share the blame for the situation with the U.S. Food and Drug Administration and pharmaceutical manufacturers which encourage doctors to use the conversion tables.
"We came up with these estimates about how to determine what would be safe," Webster said, "but they're really not scientifically based."






